

2/10—Oxford vaccine 10% effective in South Africa; Pfizer 81% to 146% in lab tests
Oxford Covid vaccine has 10% efficacy against South African variant, study suggests
[Media report.] Prof Shabir Madhi from the University of the Witwatersrand, who led the Oxford/AstraZeneca trial in South Africa, said that “The results that we now describe against the variant, the point estimate is 10%. Clearly, that is far off the 60% mark and, even if you had a larger study you are unlikely to get to a vaccine efficacy readout of even 40 or 50%.” South Africa has halted the rollout of the Oxford/AstraZeneca jab in the wake of the trial, the results of which are awaiting publication and peer review.
Neutralization of SARS-CoV-2 spike 69/70 deletion, E484K and N501Y variants by BNT162b2 vaccine-elicited sera [Pfizer]
We engineered three SARS-CoV-2 viruses containing key spike mutations from the newly emerged United Kingdom (UK) and South African (SA) variants: N501Y from UK and SA; 69/70-deletion + N501Y + D614G from UK; and E484K + N501Y + D614G from SA. Neutralization geometric mean titers (GMTs) of 20 BTN162b2 vaccine-elicited human sera against the three mutant viruses were 0.81- to 1.46-fold of the GMTs against parental virus, indicating small effects of these mutations on neutralization by sera elicited by two BNT162b2 doses.
Decreased SARS-CoV-2 viral load following vaccination [Pfizer]
[Preprint.] Beyond their substantial protection of individual vaccinees, it is hoped that the COVID-19 vaccines would reduce viral load in breakthrough infections thereby further suppress onward transmission. Here, analyzing positive SARS-CoV-2 test results following inoculation with the BNT162b2 mRNA vaccine, we find that the viral load is reduced 4-fold for infections occurring 12-28 days after the first dose of vaccine. These reduced viral loads hint to lower infectiousness, further contributing to vaccine impact on virus spread.
COVID-19 vaccines: acting on the evidence
Diverging from tested vaccination regimens without scientific evidence could undermine public confidence in vaccines against COVID-19 and the success of a global vaccination strategy to curtail the pandemic. The UK government, for example, has extended the interval between doses of the Pfizer–BioNTech mRNA vaccine from a regime of two doses scheduled 21 days apart, as tested in clinical trials, to two doses no more than 12 weeks apart. The published efficacy of the Pfizer–BioNTech vaccine was determined to be 52% between the first dose and second dose; however, post-hoc analyses using case data restricted to 15–21 days after the first dose estimated the efficacy at 89%. Vaccination policies firmly grounded in scientific evidence must remain the mainstay of the global COVID-19 exit strategy.
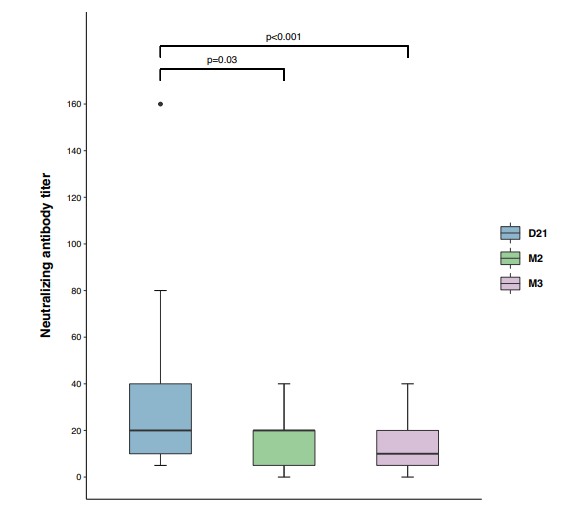
Rapid decline of neutralizing antibodies against SARS-CoV-2 among infected healthcare workers
We followed 26 healthcare workers with mild COVID-19 three weeks (D21), two months (M2) and three months (M3) after the onset of symptoms. All the healthcare workers had anti-receptor binding domain (RBD) IgA at D21, decreasing to 38.5% at M3 (p < 0.0001). This neutralizing activity declines, and may even be lost, in association with a decrease in systemic IgA antibody levels, from two months after disease onset. This short-lasting humoral protection supports strong recommendations to maintain infection prevention and control measures in healthcare workers, and suggests that periodic boosts of SARS-CoV-2 vaccination may be required.
Missed an update? View past issues.