

2/5—French study predicts vaccine acceptance 27·4% to 61·3%
COVID-19 vaccine hesitancy in a representative working-age population in France: a survey experiment based on vaccine characteristics
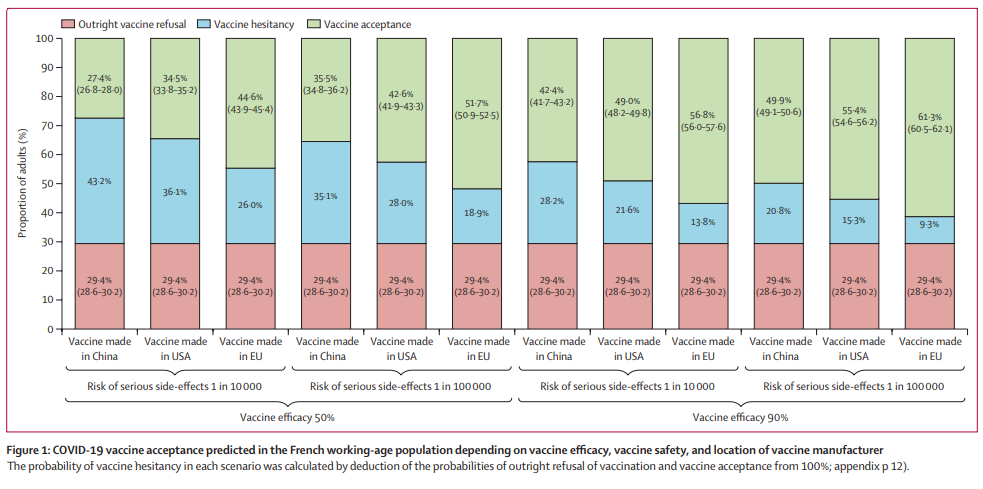
Survey responses were collected from 1942 working-age adults, of whom 560 (28·8%) opted for no vaccination in all eight tasks (outright vaccine refusal) and 1382 (71·2%) did not. Outright vaccine refusal was associated with a lower perceived severity of COVID-19, whereas vaccine hesitancy was lower when herd immunity benefits were communicated and in working versus non-working individuals, and those with experience of COVID-19 (had symptoms or knew someone with COVID-19). For a mass vaccination campaign involving mass vaccination centres and communication of herd immunity benefits, our model predicted outright vaccine refusal in 29·4% (95% CI 28·6–30·2) of the French working-age population. Predicted hesitancy was highest for vaccines manufactured in China with 50% efficacy and a 1 in 10 000 risk of serious side-effects (vaccine acceptance 27·4% [26·8–28·0]), and lowest for a vaccine manufactured in the EU with 90% efficacy and a 1 in 100 000 risk of serious side-effects (vaccine acceptance 61·3% [60·5–62·1]).
Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine (CoronaVac) in healthy adults aged 60 years and older: a randomised, double-blind, placebo-controlled, phase 1/2 clinical trial [Sinovac]
We did a randomised, double-blind, placebo-controlled, phase 1/2 clinical trial of CoronaVac in healthy adults aged 60 years and older in Renqiu (Hebei, China). Between May 22 and June 1, 2020, 72 participants (24 in each intervention group and 24 in the placebo group; mean age 65·8 years [SD 4·8]) were enrolled in phase 1, and between June 12 and June 15, 2020, 350 participants were enrolled in phase 2 (100 in each intervention group and 50 in the placebo group; mean age 66·6 years [SD 4·7] in 349 participants). In the safety populations from both phases, any adverse reaction within 28 days after injection occurred in 20 (20%) of 100 participants in the 1·5 μg group, 25 (20%) of 125 in the 3 μg group, 27 (22%) of 123 in the 6 μg group, and 15 (21%) of 73 in the placebo group. All adverse reactions were mild or moderate in severity and injection site pain (39 [9%] of 421 participants) was the most frequently reported event. As of Aug 28, 2020, eight serious adverse events, considered unrelated to vaccination, have been reported by seven (2%) participants. In phase 1, seroconversion after the second dose was observed in 24 of 24 participants (100·0% [95% CI 85·8–100·0]) in the 3 μg group and 22 of 23 (95·7% [78·1–99·9]) in the 6 μg group. In phase 2, seroconversion was seen in 88 of 97 participants in the 1·5 μg group (90·7% [83·1–95·7]), 96 of 98 in the 3 μg group (98·0% [92·8–99·8]), and 97 of 98 (99·0% [94·5–100·0]) in the 6 μg group. CoronaVac is safe and well tolerated in older adults. Neutralising antibody titres induced by the 3 μg dose were similar to those of the 6 μg dose, and higher than those of the 1·5 μg dose, supporting the use of the 3 μg dose CoronaVac in phase 3 trials to assess protection against COVID-19.
Inactivated COVID-19 vaccines to make a global impact
Because of the ease of production and scale-up and relatively low cost, inactivated vaccines can capture a sizeable portion of the SARS-CoV-2 vaccine landscape. Inactivated vaccines are well established and can provide advantages in a variety of distinct populations, including those with degrees of immune senescence. Compared with other vaccines targeting only the spike protein, inactivated vaccines could provide an added benefit to these individuals by boosting their T-cell responses against many of the SARS-CoV-2 proteins.
Comparative cost-effectiveness of SARS-CoV-2 testing strategies in the USA: a modelling study
Our modelling showed that daily testing combined with a 2-week isolation period was the most costly strategy considered, reflecting increased costs with greater test frequency and length of isolation period. Assuming a societal willingness to pay of US$100 000 per YLL averted and a price of $5 per test, the strategy most likely to be cost-effective under a rapid transmission scenario (Re of 2·2) is weekly testing followed by a 2-week isolation period subsequent to a positive test result. Under low transmission scenarios (Re of 1·2), monthly testing of the population followed by 1-week isolation rather than 2-week isolation is likely to be most cost-effective. Resources recouped from shortened isolation duration could be cost-effectively allocated to more frequent testing.
Calling for benefit–risk evaluations of COVID-19 control measures
Compared with a historical baseline, UK nursing homes and hospices saw an increase in the number of deaths between February and June, 2020, associated with acute coronary syndrome (a 41% increase), stroke (a 39% increase), and heart failure (a 25% increase). The situation is similar for patients with cancer. In German hospitals, cancer cases decreased during the first national lockdown, suggesting that cancers might have been undetected and untreated during this period. In England, hospital admissions for chemotherapy appointments have fallen by 60% […] which could contribute to 6270 additional deaths within 1 year. Government restrictions are disrupting traditional means of support between friends and family members. While trying to control COVID-19, all aspects of physical and mental health need to be jointly considered. Other life-threatening diseases are being neglected, and patients with these diseases should receive the same timely and appropriate medical treatment as patients with COVID-19.
Missed an update? View past issues.