3/24—Vaccine response in pregnant and lactating women: a cohort study
COVID-19 vaccine response in pregnant and lactating women: a cohort study
[Preprint.] 131 reproductive-age vaccine recipients (84 pregnant, 31 lactating, and 16 non-pregnant) were enrolled. Vaccine-induced immune responses were equivalent in pregnant and lactating vs non-pregnant women. All titers were higher than those induced by SARS-CoV-2 infection during pregnancy. Vaccine-generated antibodies were present in all umbilical cord blood and breastmilk samples. SARS-CoV-2 specific IgG, but not IgA, increased in maternal blood and breastmilk with vaccine boost. Immune transfer to neonates occurred via placental and breastmilk.
AZD1222 US Phase III trial met primary efficacy endpoint in preventing COVID-19 at interim analysis
[Press release. Via Johns Hopkins.] The trial included more than 32,000 participants in Chile, Peru, and the US, including 21,583 who received at least one dose of the vaccine. The press release reports an overall efficacy of 79% against any COVID-19 disease among all age groups and 80% efficacy for adults aged 65 years and older. Additionally, the press release describes 100% efficacy against severe disease and hospitalization. AstraZeneca explicitly noted that an independent review of the safety data “found no increased risk of thrombosis or events characterised by thrombosis” associated with the vaccine.
Efficacy of the ChAdOx1 nCoV-19 Covid-19 Vaccine against the B.1.351 Variant [AstraZeneca]
Between June 24 and November 9, 2020, we enrolled 2026 HIV-negative adults (median age, 30 years); 1010 and 1011 participants received at least one dose of placebo or vaccine, respectively. Both the pseudovirus and the live-virus neutralization assays showed greater resistance to the B.1.351 variant in serum samples obtained from vaccine recipients than in samples from placebo recipients. In the primary end-point analysis, mild-to-moderate Covid-19 developed in 23 of 717 placebo recipients (3.2%) and in 19 of 750 vaccine recipients (2.5%), for an efficacy of 21.9% (95% confidence interval [CI], −49.9 to 59.8). Among the 42 participants with Covid-19, 39 cases (92.9%) were caused by the B.1.351 variant; vaccine efficacy against this variant, analyzed as a secondary end point, was 10.4% (95% CI, −76.8 to 54.8). A two-dose regimen of the ChAdOx1 nCoV-19 vaccine did not show protection against mild-to-moderate Covid-19 due to the B.1.351 variant.
Longitudinal analysis of humoral immunity against SARS-CoV-2 Spike in convalescent individuals up to 8 months post-symptom onset
[Preprint.] Since the absence of antibodies does not equate to absence of immune memory, we sought to determine the presence of SARS-CoV-2-specific memory B cells in COVID-19 convalescent patients. In this study, we report on the evolution of the overall humoral immune responses on 101 blood samples obtained from 32 COVID-19 convalescent patients between 16 and 233 days post-symptom onset. Our observations indicate that anti-Spike and anti-RBD IgM in plasma decay rapidly, whereas the reduction of IgG is less prominent. The number of IgG+ memory B cells remain stable for up to 8 months after symptoms onset.
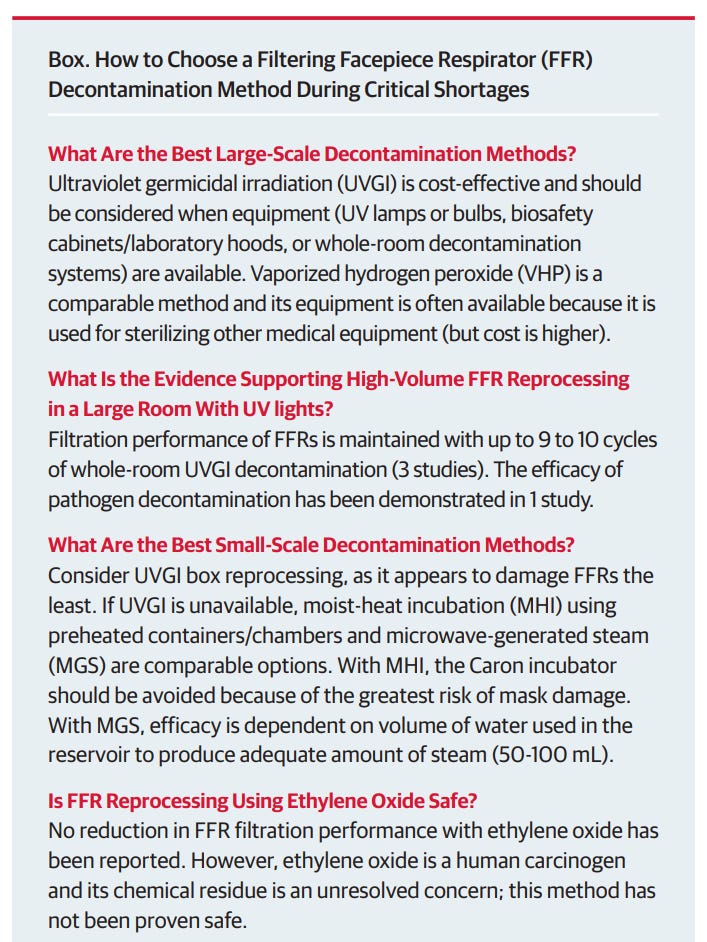
Filtering Facepiece Respirator (N95 Respirator) Reprocessing: A Systematic Review
A search of PubMed and EMBASE (through January 31, 2021) was completed for 5 types of respirator-decontaminating processes. Forty-two studies were included that examined 65 total types of masks. All were laboratory studies (no clinical trials), and 2 evaluated respirator performance and fit with actual clinical use of N95 respirators. Ultraviolet germicidal irradiation, vaporized hydrogen peroxide, moist heat, and microwave-generated steam processing effectively sterilized N95 respirators and retained filtration performance. Ultraviolet irradiation and vaporized hydrogen peroxide damaged respirators the least. More research is needed on decontamination effectiveness for SARS-CoV-2 because few studies specifically examined this pathogen.