627,383 vaccinated in the UK: side-effects & infections
Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: a prospective observational study
Between Dec 8, and March 10, 2021, 627 383 individuals reported being vaccinated with 655 590 doses: 282 103 received one dose of BNT162b2, of whom 28 207 received a second dose, and 345 280 received one dose of ChAdOx1 nCoV-19. Systemic side-effects were reported by 13·5% (38 155 of 282 103) of individuals after the first dose of BNT162b2, by 22·0% (6216 of 28 207) after the second dose of BNT162b2, and by 33·7% (116 473 of 345 280) after the first dose of ChAdOx1 nCoV-19. Systemic side-effects were more common (1·6 times after the first dose of ChAdOx1 nCoV-19 and 2·9 times after the first dose of BNT162b2) among individuals with previous SARS-CoV-2 infection than among those without known past infection. Local effects were similarly higher in individuals previously infected than in those without known past infection. 3106 of 103 622 vaccinated individuals and 50 340 of 464 356 unvaccinated controls tested positive for SARS-CoV-2 infection. Significant reductions in infection risk were seen starting at 12 days after the first dose, reaching 60% (95% CI 49–68) for ChAdOx1 nCoV-19 and 69% (66–72) for BNT162b2 at 21–44 days and 72% (63–79) for BNT162b2 after 45–59 days.
Children develop strong and sustained cross-reactive immune responses against Spike protein following SARS-CoV-2 infection, with enhanced recognition of variants of concern
[Preprint.] We studied the profile of antibody and cellular immunity in children aged 3-11 years in comparison with adults. Antibody profiles in children were strong, with high titres against Spike protein and receptor binding domain (RBD). SARS-CoV-2 seroconversion in children strongly boosted antibody responses against seasonal beta-coronaviruses, partly through cross-recognition of the S2 domain, indicating a broad humoral response that was not seen in adults. T cell responses against Spike were also >2-fold higher in children compared to adults and displayed a strong Th1 cytokine profile. Children thus distinctly generate robust, cross-reactive and sustained immune responses after SARS-CoV-2 infection, with focussed specificity against Spike protein.
A guideline to limit indoor airborne transmission of COVID-19
Social distancing, specifically the Six-Foot Rule, offers little protection from pathogen-bearing aerosol droplets sufficiently small to be continuously mixed through an indoor space. We here build on models of airborne disease transmission in order to derive an indoor safety guideline that would impose an upper bound on the “cumulative exposure time,” the product of the number of occupants and their time in an enclosed space. We demonstrate how this bound depends on the rates of ventilation and air filtration, dimensions of the room, breathing rate, respiratory activity and face mask use of its occupants, and infectiousness of the respiratory aerosols. By synthesizing available data from the best-characterized indoor spreading events with respiratory drop size distributions, we estimate an infectious dose on the order of 10 aerosol-borne virions. Case studies are presented for classrooms and nursing homes, and a spreadsheet and online app are provided to facilitate use of our guideline.
Characteristics of SARS-CoV-2 variants of concern B.1.1.7, B.1.351 or P.1: data from seven EU/EEA countries, weeks 38/2020 to 10/2021
We compared 19,207 cases of SARS-CoV-2 variant B.1.1.7/S gene target failure (SGTF), 436 B.1.351 and 352 P.1 to non-variant cases reported by seven European countries. COVID-19 cases with these variants had significantly higher adjusted odds ratios for hospitalisation (B.1.1.7/SGTF: 1.7, 95% confidence interval (CI): 1.0–2.9; B.1.351: 3.6, 95% CI: 2.1–6.2; P.1: 2.6, 95% CI: 1.4–4.8) and B.1.1.7/SGTF and P.1 cases also for intensive care admission (B.1.1.7/SGTF: 2.3, 95% CI: 1.4–3.5; P.1: 2.2, 95% CI: 1.7–2.8).
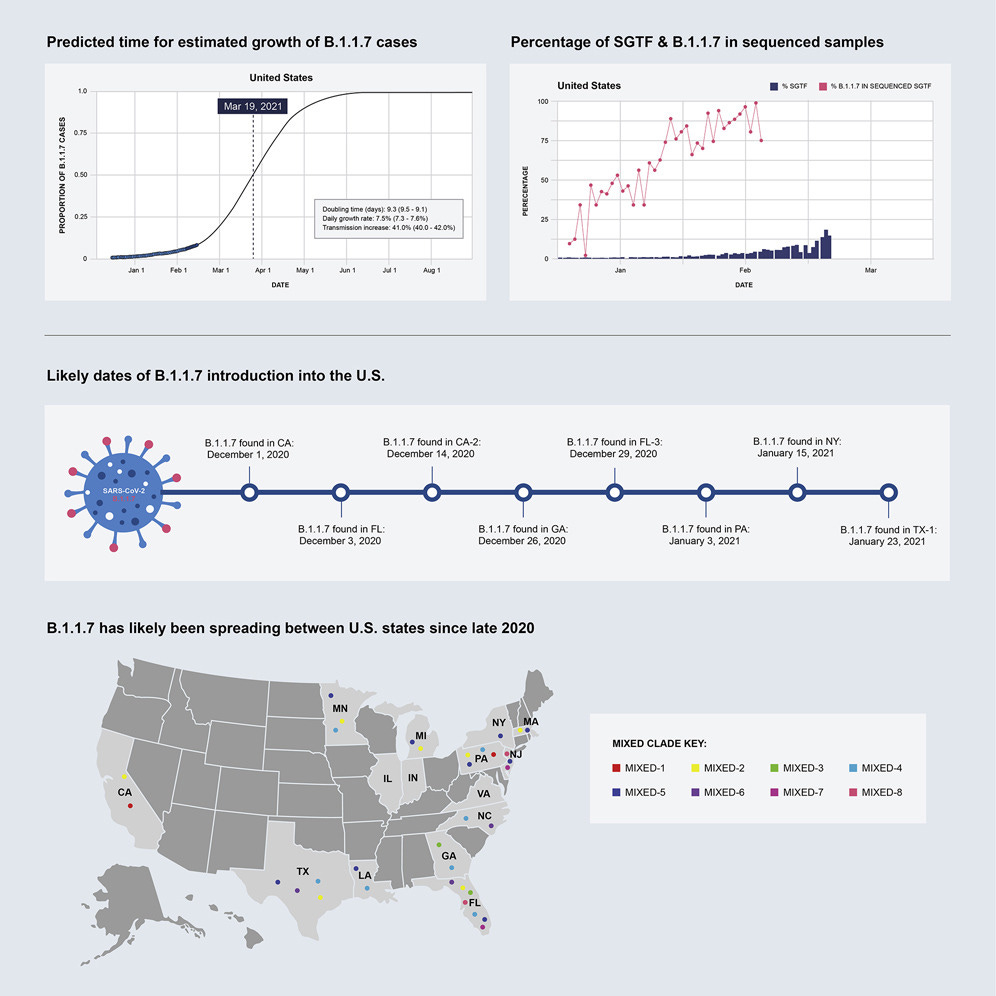
Emergence and rapid transmission of SARS-CoV-2 B.1.1.7 in the United States
We found that, while the fraction of B.1.1.7 varied by state, the variant increased at a logistic rate with a roughly weekly doubling rate and an increased transmission of 40%–50%. We revealed several independent introductions of B.1.1.7 into the US as early as late November 2020, with community transmission spreading it to most states within months. We show that the US is on a similar trajectory as other countries where B.1.1.7 became dominant, requiring immediate and decisive action to minimize COVID-19 morbidity and mortality.