

8/28—2 m or 1: what is the evidence for physical distancing?
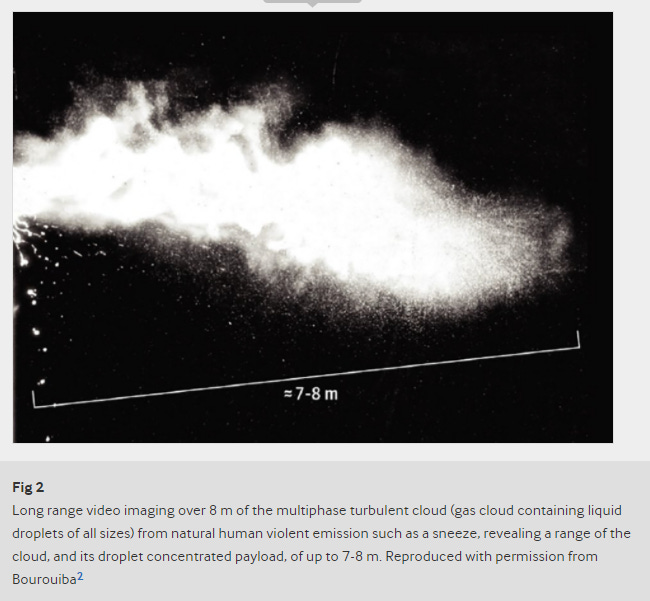
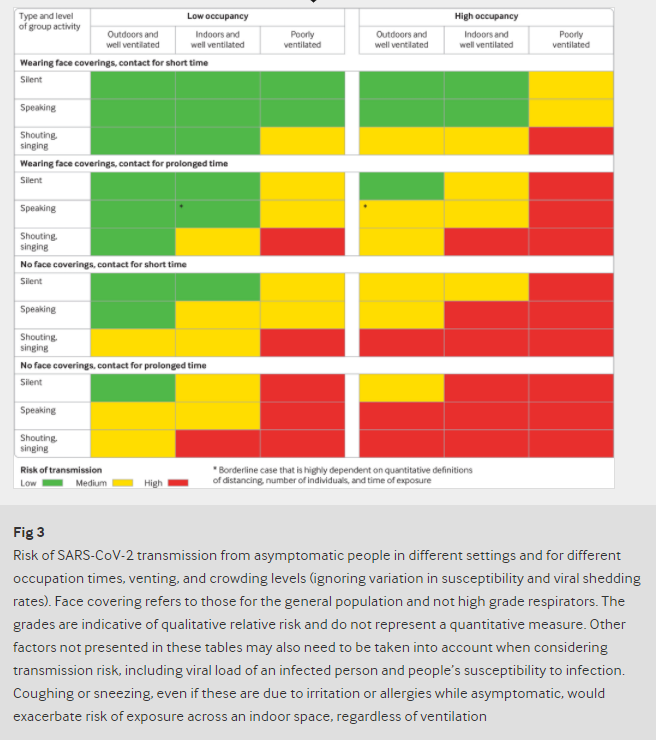
Rules that stipulate a single specific physical distance (1 or 2 metres) between individuals to reduce transmission of SARS-CoV-2, the virus causing covid-19, are based on an outdated, dichotomous notion of respiratory droplet size. After the cloud slows sufficiently, ventilation, specific patterns of airflow, and type of activity become important. Viral load of the emitter, duration of exposure, and susceptibility of an individual to infection are also important (Jones et al. 2020).
Virus transmission from urinals
Similar to the toilet-induced flushing, results indicate that the trajectory of the particles triggered by the urinal flushing manifests an external spread type. Even more alarmingly, the particle can reach 0.84 m (man’s thigh) in 5.5 s when compared with the diffusion performance of the toilet-induced one (around 0.93 m in 35 s). Wearing masks should be made mandatory in public washrooms, and anti-diffusion improvements of facilities in public washrooms are urgently needed.
Social Distancing during the COVID‐19 Pandemic: Who Are the Present and Future Noncompliers?
Using survey data from a sample of U.S. residents (n = 1,449), the authors show that some demographic factors (gender, age, race, political party) help predict intent to adhere to social distancing. Women report higher levels of social distancing than men. Black individuals appear to socially distance somewhat less than others do, and Asians appear to socially distance slightly more. Education appears to have little association with social distancing. Those who primarily get their news from radio or social media tend to report slightly less social distancing, while those who primarily get their news from websites tend to report more. Those who believe that COVID‐19 is a monumental threat to society tend to socially distance more. Those who think we must keep the economy going even if it means more COVID‐19 deaths report behavior less consistent with social distancing guidelines.
Adherence to Personal Protective Equipment Guidelines During the COVID‐19 Pandemic: A Worldwide Survey Study
From April 17 to June 17, 2020, 1255 surveys were completed. Respondents included physicians (43·8%), nurses (29·6%), midwives (19·8%), paramedics (3·8%) and technicians (3·1%). At the country level, Japan (100%) showed the highest adherence in communal hospital spaces. Highest adherence was mostly noted in European countries (UK, 85%, patient contact when COVID‐19 not suspected; Spain, 81·3%, patient contact when COVID‐19 suspected; Portugal, 81·5%, patient contact with confirmed cases). Exceptions, were Argentina (83·3%) when carrying out AGPs and China (71·5%) in high‐risk areas. Lowest adherence was noted in Norway in communal hospital spaces (6·9%) and patient contact when COVID‐19 not suspected (10·3%), and Germany when carrying out AGPs (13·6%) and in high risk areas (18·2%). Finally, Canada showed the lowest adherence during patient contact when COVID‐19 is suspected (15·2%) or confirmed (26·6%). The reasons for this variability are multifactorial, including PPE shortages disproportionately affecting countries, forcing healthcare institutions to resort to alternative approaches, such as decontamination and re‐use.
Transmission of COVID-19 in school settings and interventions to reduce the transmission: a rapid review
This review included 9 studies: 3 epidemiological and 6 modelling studies (including 5 preprints) (search up to 18 June 2020). There is limited and weak evidence from the 3 epidemiological studies that the transmission of COVID-19 within school settings is low. There is weak evidence from 6 modelling studies that the re-opening of schools at a reduced capacity, particularly for younger children, may not be associated with a second epidemic wave.
Get it by email:
Missed an update? View past issues.