"Around 50% to 60% reduced risk" of infection when fully vaccinated
Coronavirus infections three times lower in double vaccinated people
[Imperial College London news report.] People who were unvaccinated had a three-fold higher prevalence than those who had received both doses of a vaccine, at 1.21% compared to 0.40%. However both of these represent more than a five-fold increase compared to the previous round (0.24%, 0.07%, respectively). Based on these data, the researchers estimate that fully vaccinated people in this testing round had between around 50% to 60% reduced risk of infection, including asymptomatic infection, compared to unvaccinated people. In addition, double vaccinated people were less likely than unvaccinated people to test positive after coming into contact with someone who had COVID-19 (3.84% vs 7.23%).
REACT-1 round 13 final report: exponential growth, high prevalence of SARS-CoV-2 and vaccine effectiveness associated with Delta variant in England during May to July 2021
[Preprint.] We analysed prevalence trends and their drivers using reverse transcription-polymerase chain reaction (RT-PCR) swab-positivity data from round 12 (between 20 May and 7 June 2021) and round 13 (between 24 June and 12 July 2021). We observed sustained exponential growth with an average doubling time in round 13 of 25 days (lower Credible Interval of 15 days) and an increase in average prevalence from 0.15% (0.12%, 0.18%) in round 12 to 0.63% (0.57%, 0.18%) in round 13. However, in round 13, 44% of infections occurred in fully vaccinated individuals, reflecting imperfect vaccine effectiveness against infection despite high overall levels of vaccination. Using self-reported vaccination status, we estimated adjusted vaccine effectiveness against infection in round 13 of 49% (22%, 67%) among participants aged 18 to 64 years. We estimated adjusted vaccine effectiveness against symptomatic infection of 59% (23%, 78%). Increased mixing during the autumn in the presence of the Delta variant may lead to renewed growth, even at high levels of vaccination.
COVID-19 rapid guideline: vaccine-induced immune thrombocytopenia and thrombosis (VITT)
[UK NICE guidelines, via BMJ news.] Patients who are acutely unwell with suspected vaccine induced immune thrombocytopenia and thrombosis (VITT) should be referred immediately to the emergency department. Although VITT is extremely rare, with 14.2 cases per million doses of a covid-19 vaccine, the condition requires swift diagnosis and urgent treatment.
Dominance of Alpha and Iota variants in SARS-CoV-2 vaccine breakthrough infections in New York City
[Preprint.] We compared the SARS-CoV-2 genomes of 76 breakthrough cases after full vaccination with BNT162b2 (Pfizer/BioNTech), mRNA-1273 (Moderna), or JNJ-78436735 (Janssen) to unvaccinated controls (February-April 2021) in metropolitan New York. Most breakthrough infections (57/76) occurred with B.1.1.7 (Alpha) or B.1.526 (Iota). Among the 7 hospitalized cases, 4 were infected with B.1.1.7, including 1 death. Both unmatched and matched statistical analyses considering age, sex, vaccine type, and study month as covariates supported the null hypothesis of equal variant distributions between vaccinated and unvaccinated in chi-squared and McNemar tests (p>0.1) highlighting a high vaccine efficacy against B.1.1.7 and B.1.526. The evolving dynamic of SARS-CoV-2 variants requires broad genomic analyses of breakthrough infections to provide real-life information on immune escape mediated by circulating variants and their spike mutations.
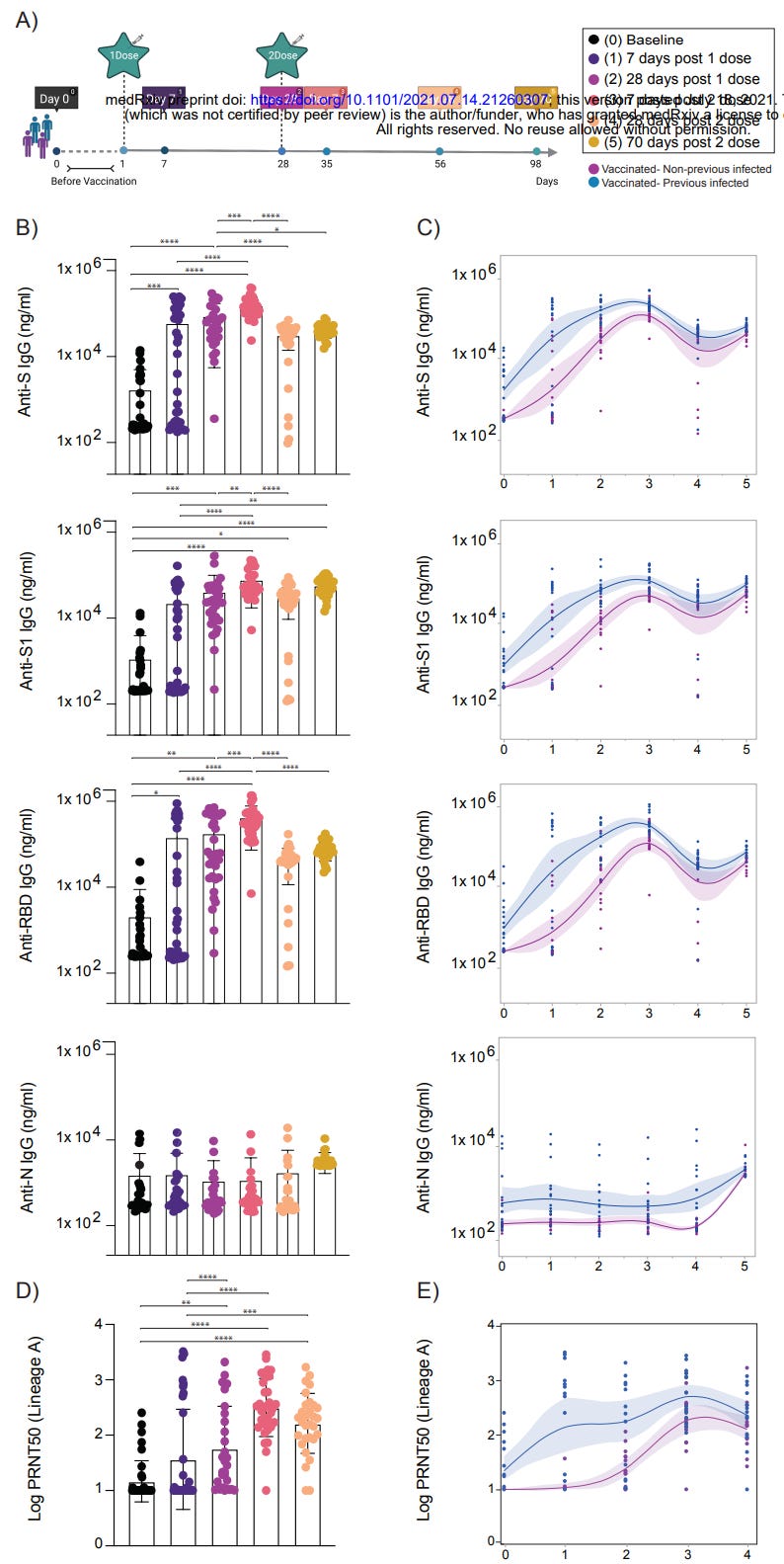
Impact of circulating SARS-CoV-2 variants on mRNA vaccine-induced immunity in uninfected and previously infected individuals
[Preprint.] We analysed the development of anti-SARS-CoV-2 antibody and T cell responses in previously infected (recovered) or uninfected (naive) individuals that received mRNA vaccines to SARS-CoV-2. Comprehensive analysis of plasma neutralization using 16 authentic isolates of distinct locally circulating SARS-CoV-2 variants revealed a range of reduction in the neutralization capacity associated with specific mutations in the spike gene: lineages with E484K and N501Y/T (e.g., B.1.351 and P.1) had the greatest reduction, followed by lineages with L452R (e.g., B.1.617.2) or with E484K (without N501Y/T). While both groups retained neutralization capacity against all variants, plasma from previously infected vaccinated individuals displayed overall better neutralization capacity when compared to plasma from uninfected individuals that also received two vaccine doses, pointing to vaccine boosters as a relevant future strategy to alleviate the impact of emerging variants on antibody neutralizing activity.