Effectiveness of vaccination: systematic review and meta-analysis
Effectiveness of vaccination against symptomatic and asymptomatic SARS-CoV-2 infection: a systematic review and meta-analysis
[Preprint. Studies included up to May 15, 2021.] The evaluation was narrowed to two mRNA vaccines and two modified adenovirus vectored vaccines. The overall risk of SARS-CoV-2 infection confirmed by real time Polymerase Chain Reaction (PCR) was estimated in partially and fully vaccinated individuals. The effect size was expressed as Relative Risk (RR) and RRR (RR reduction) of SARS-CoV-2 infection after vaccination. The systematic review identified 27 studies eligible for the quantitative synthesis. Partially vaccinated individuals presented a RRR=73% (95%CI=59%-83%) for any positive SARS-CoV-2 PCR (RR=0.27) and a RRR=79% (95%CI=30%-93%) for symptomatic SARS-CoV-2 PCR (RR=0.21). Fully vaccinated individuals showed a RRR=94% (95%CI=88%-98%) for any SARS-CoV-2 positive PCR (RR=0.06) compared to unvaccinated. According to the subgroup meta-analysis, full BNT162b2 vaccination protocol achieved a RRR=84%-94% against any SARS-CoV-2 positive PCR and a RRR=68%-84% against symptomatic positive PCR. The RR for any SARS-CoV-2 positive PCR remained higher within elderly groups aged ≥69 years (RR=0.12-0.15) compared to younger individuals (RR=0.05-0.12). The RR against B.1.351 infection approached 0.40 for any positive PCR and 0.36 for symptomatic SARS-COV-2 while the RR of any B.1.1.7 infection was 0.14.
Factors Associated With Household Transmission of SARS-CoV-2
An Updated Systematic Review and Meta-analysis
In this updated systematic review and meta-analysis of 87 studies representing 1 249 163 household contacts from 30 countries, the estimated household secondary attack rate was 19%. An increase in household transmission was observed over time, perhaps owing to improved diagnostic procedures and tools, longer follow-up, more contagious variants, and different study locations.
Evolution of antibody responses up to 13 months after SARS-CoV-2 infection and risk of reinfection
This is a prospective, monocentric, longitudinal, cohort clinical study. Healthcare workers (HCW) from Strasbourg University Hospital were enrolled between April 6th and May 7th, 2020 and followed up to 422 days. A total of 4290 samples from 393 convalescent COVID-19 and 916 COVID-19 negative individuals were analyzed. In convalescent individuals, SARS-CoV-2 antibodies followed a triphasic kinetic model with half-lives at month (M) 11–13 of 283 days (95% CI 231–349) for anti-N and 725 days (95% CI 623–921) for anti-RBD IgG, which stabilized at a median of 1.54 log BAU/mL (95% CI 1.42–1.67). The incidence of SARS-CoV-2 infections was 12.22 and 0.40 per 100 person-years in COVID-19-negative and COVID-19-positive HCW, respectively, indicating a relative reduction in the incidence of SARS-CoV-2 reinfection of 96.7%. Our study demonstrates a long-term persistence of anti-RBD antibodies that may reduce risk of reinfection.
Lessons from the covid-19 third wave in canada: the impact of variants of concern and shifting demographics
[Preprint.] Compared to the 372,741 individuals with SARS-CoV-2 infection between March 2020 and January 2021 (waves 1 and 2 in Canada), there was a shift in transmission towards younger patients in the 104,232 COVID-19 cases identified in wave 3. As a result, although third wave patients were more likely to be hospitalized (aOR 1.34 [1.29-1.39] in Ontario and aOR 1.53 [95%CI 1.41-1.65] in Alberta), they had shorter lengths of stay (median 5 vs. 7 days, p<0.001) and were less likely to die within 30 days (aOR 0.66 [0.60-0.71] in Ontario and aOR 0.74 [0.62-0.89] in Alberta). However, within the third wave, patients infected with VOC (91% Alpha) exhibited higher risks of death (aOR 1.52 [1.27-1.81] in Ontario and aOR 1.67 [1.13-2.48] in Alberta) and hospitalization (aOR 1.57 [1.47-1.69] in Ontario and aOR 1.88 [1.74-2.02] in Alberta) than those with wild-type SARS-CoV-2 infections during the same timeframe. On a population basis, the shift towards younger age groups as the COVID-19 pandemic has evolved translates into more hospitalizations but shorter lengths of stay and lower mortality risk than seen in the first 10 months of the pandemic in Canada. However, on an individual basis, infection with a VOC is associated with a higher risk of hospitalization or death than the original wild-type SARS-CoV-2.
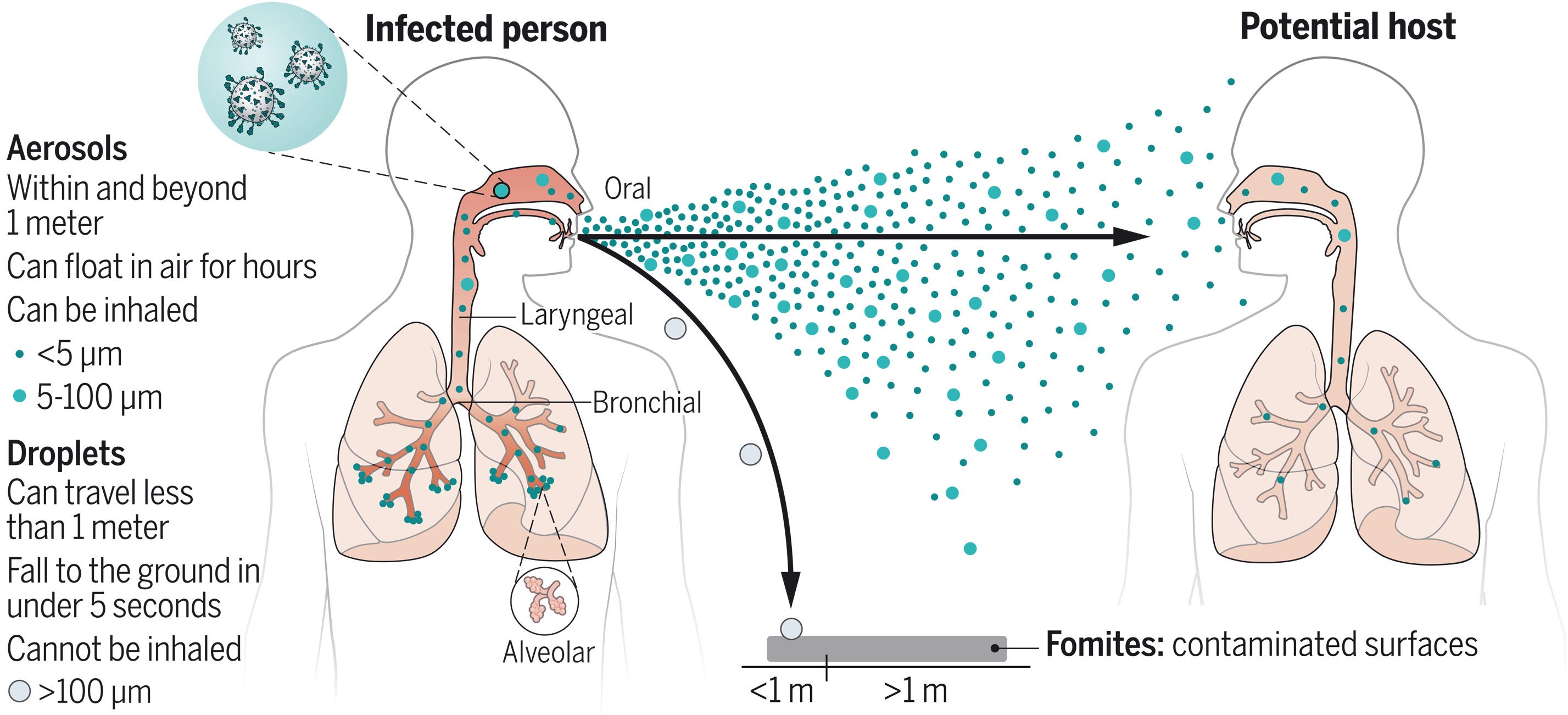
Airborne transmission of respiratory viruses
Traditionally, it was thought that respiratory pathogens spread between people through large droplets produced in coughs and through contact with contaminated surfaces (fomites). However, several respiratory pathogens are known to spread through small respiratory aerosols, which can float and travel in air flows, infecting people who inhale them at short and long distances from the infected person. The authors suggest that airborne transmission may be the dominant form of transmission for several respiratory pathogens, including SARS-CoV-2, and that further understanding of the mechanisms underlying infection from the airborne route will better inform mitigation measures.