Recovered individuals who continued to test positive were not infectious to others
SARS-CoV-2 Transmission Risk Among National Basketball Association Players, Staff, and Vendors Exposed to Individuals With Positive Test Results After COVID-19 Recovery During the 2020 Regular and Postseason
This retrospective cohort study used data collected from June 11, 2020, to October 19, 2020, as part of the National Basketball Association (NBA) closed campus occupational health program in Orlando, Florida, which required daily RT-PCR testing and ad hoc serological testing for SARS-CoV-2 IgG antibodies. Among 3648 individuals who participated, 36 (1%) were persistent positive cases, most of whom were younger than 30 years (24 [67%]) and male (34 [94%]). Antibodies were detected in 33 individuals (91.7%); all remained asymptomatic following the index persistent positive RT-PCR result. Cases were monitored for up to 100 days (mean [SD], 51 [23.9] days), during which there were at least 1480 person-days of direct exposure activities, with no transmission events or secondary infections of SARS-CoV-2 detected (0 new cases).
SARS-CoV-2 transmission without symptoms
It is virtually impossible to detect such cases without continuous community surveillance screening, which has not been widely implemented, or without effective contact tracing and testing. Early studies reported that asymptomatic cases accounted for 30 to 80% of infections, but more recent data point to a rate of asymptomatic cases between 17 and 30%. The biological basis for transmission without symptoms is poorly understood. Symptomless transmission is influenced by the timing and magnitude of the host response to infection, which is a major determinant of pathogenicity. For presymptomatic cases, research has shown that viral shedding is highest just before and for a few days after symptoms begin, which is a critical time to ensure that individuals who may not realize they have been exposed stay home when possible and practice risk reduction efforts when in the community.
Resurgence of SARS-CoV-2: detection by community viral surveillance
Surveillance of the SARS-CoV-2 epidemic has mainly relied on case reporting which is biased by health service performance, test availability and test-seeking behaviors. We report a community-wide national representative surveillance program in England involving self-administered swab results from 594,000 individuals tested for SARS-CoV-2, regardless of symptoms, from May to beginning of September 2020. The epidemic declined between May and July 2020 but then increased gradually from mid-August, accelerating into early September 2020 at the start of the second wave. When compared to cases detected through routine surveillance, we report here a longer period of decline and a younger age distribution. Representative community sampling for SARS-CoV-2 can substantially improve situational awareness and feed into the public health response even at low prevalence.
Household COVID-19 risk and in-person schooling
Data from a massive online survey in the United States indicates an increased risk of COVID-19-related outcomes among respondents living with a child attending school in-person. School-based mitigation measures are associated with significant reductions in risk, particularly daily symptoms screens, teacher masking, and closure of extra-curricular activities. A positive association between in-person schooling and COVID-19 outcomes persists at low levels of mitigation, but when seven or more mitigation measures are reported, a significant relationship is no longer observed. Among teachers, working outside the home was associated with an increase in COVID-19-related outcomes, but this association is similar to other occupations (e.g., healthcare, office work).
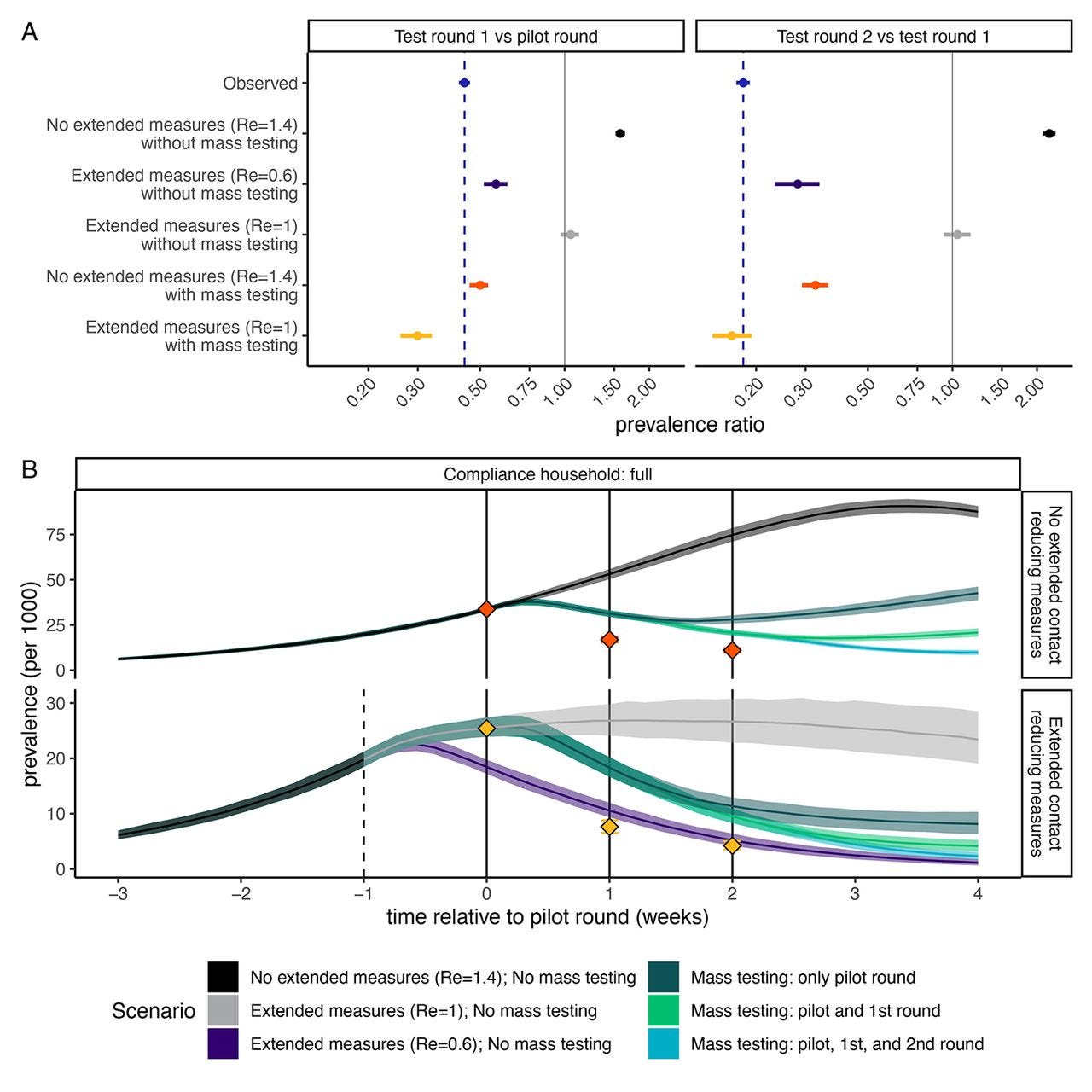
The impact of population-wide rapid antigen testing on SARS-CoV-2 prevalence in Slovakia
Slovakia conducted multiple rounds of population-wide rapid antigen testing for SARS-CoV-2 in late 2020, combined with a period of additional contact restrictions. Observed prevalence decreased by 58% (95% CI: 57-58%) within one week in the 45 counties that were subject to two rounds of mass testing, an estimate that remained robust when adjusting for multiple potential confounders. Adjusting for epidemic growth of 4.4% (1.1-6.9%) per day preceding the mass testing campaign, the estimated decrease in prevalence compared to a scenario of unmitigated growth was 70% (67-73%). Modelling indicated that this decrease could not be explained solely by infection control measures, but required the additional impact of isolation and quarantine of household members of those testing positive.